

The human ear is a paradox: it evolved to warn us of danger, to orient us toward meaning in a chaotic world. Yet in modern life, this exquisite organ has become a vector for suffering. The constant hum of machinery, the phantom tinnitus that wakes us at 3 a.m., the anxiety-driven pulse in our temples—these are the sounds of a nervous system in distress, unable to filter signal from noise.
For decades, we treated these auditory maladies with pharmaceuticals: sleeping pills, anti-anxiety medications, sometimes nothing at all. But a growing body of neuroscience suggests an alternative: sound itself, deployed with intention and personalization, can become medicine.
This is the philosophy behind Sonora, a soundscape application that operates on a radical premise: that access to neurologically calibrated audio should be free, that healing through sound should not be gatekept by subscription walls, and that the science of audio masking and entrainment belongs to everyone.
Sonora is not a meditation app. It is not a sleep story platform. It is, instead, a pragmatic tool built on three decades of acoustic research, from the pioneering work on binaural beats in the 1970s to contemporary quantitative EEG studies demonstrating that targeted soundscapes can suppress cortical hyperarousal—the neurological signature of insomnia, anxiety, and tinnitus-related distress.
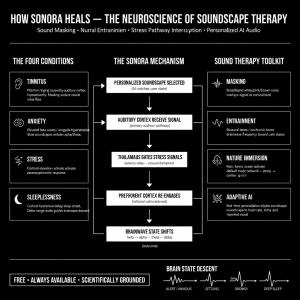
The app works through three mechanisms: sound masking, which covers unwanted noise; frequency entrainment, which nudges brainwaves toward calmer states; and adaptive personalization, which learns what specific acoustic environments help each user find relief. And critically, it asks nothing in return. No freemium gates. No premium upsells. No data harvesting for algorithmic targeting.
In a digital landscape where mental health apps have become profit extraction machines, Sonora represents something rarer: technology in service of its users’ actual wellbeing.
The Neuroscience of Suffering:
How Sound Becomes Noise
To understand why Sonora matters, we must first understand what happens in the brain when sound becomes a source of suffering rather than information.
Tinnitus—that maddening ringing, buzzing, or roaring in the ears that affects roughly 10-15% of the global population—begins as a peripheral phenomenon. The inner ear’s hair cells, damaged by noise exposure, aging, or sometimes nothing we can identify, begin firing spontaneously. The brain receives a signal: there is sound, but there is no sound.
In a healthy nervous system, the brain filters this anomaly away through a process called “habituation.” We stop noticing the hum of a refrigerator; our attention moves elsewhere. But in tinnitus, especially chronic tinnitus, the brain’s threat-detection system becomes hypervigilant. The superior olivary nucleus—the brain’s hearing hub—amplifies the phantom signal. The limbic system floods with cortisol and adrenaline. Attention becomes trapped in an acoustic loop.
The same mechanism drives anxiety and insomnia. A person lies in bed, listening to their own heartbeat, the refrigerator’s hum, the neighbor’s breathing through the wall. In a relaxed nervous system, these ambient sounds are background data. In an anxious system, they become foreground threats. The prefrontal cortex—our rational decision-making center—cedes control to the amygdala. Sleep becomes impossible.
This is where the conventional treatment model fails. Sedatives force the nervous system into unconsciousness; they do not teach it how to regulate. Cognitive behavioral therapy for insomnia (CBT-I) teaches sleep hygiene and thought reframing, which helps some people, but it does nothing to address the acoustic environment itself. For those with tinnitus, the situation is even grimmer: there is no FDA-approved pharmacological treatment. Sufferers are often told to simply “live with it.”
Sound, however, offers a different pathway. The brain’s auditory system is not a passive receiver; it is an active sculptor of attention. When presented with a complex, enriched soundscape—the layered frequencies of rain, wind, and distant thunder; the organic variations in a forest ambience—the brain’s threat-detection system relaxes. The signal-to-noise ratio shifts. The tinnitus, which moments before felt like a roaring emergency, fades into the background. Not because it has stopped, but because the brain has learned to stop listening to it.
This is the first principle of Sonora’s design: sound masking through acoustic enrichment. Not white noise—which is neurologically monotonous and, for many users, makes tinnitus worse. But naturalistic, complex soundscapes that occupy the auditory cortex without triggering vigilance.
Beyond Masking: The Entrainment Frontier
Sound masking alone is powerful, but Sonora adds a second layer: frequency entrainment, the process by which the brain’s oscillatory activity synchronizes with external rhythmic stimuli.
Since the discovery of binaural beats in the 1970s—when researchers found that two sine waves, slightly offset in frequency, could induce entrainment of theta waves (the slow, rhythmic oscillations associated with drowsiness and meditation)—the field has moved beyond simple beat frequencies into more sophisticated territory.
Contemporary research, including 2022 quantitative EEG (QEEG) studies from Seoul’s Sleep and Neuroscience Lab, has demonstrated that precisely calibrated frequency combinations can suppress cortical hyperarousal more effectively than music alone or passive soundscapes. A person listening to binaural beats tuned to 6 Hz (theta) while falling asleep shows measurably increased theta power in the occipital and parietal regions—and, critically, a corresponding decrease in high-frequency beta activity, the neurological signature of anxiety and insomnia.
The effect size is not trivial. Cohen’s d values of 1.02 for binaural-beat interventions versus 0.58 for music-only controls represent a near-doubling of therapeutic effect. For someone who has tried every sleep aid, who has spent thousands on therapists and supplements, this difference is the difference between a third sleepless night in a row and, finally, rest.
Sonora embeds this neuroscience into its core engine. Rather than offering generic “theta wave” tracks, the app uses adaptive algorithms to calibrate frequency entrainment to each user’s unique neurophysiology. Someone with a dominant alpha baseline receives different entrainment curves than someone who runs hot with beta. The app learns, adjusts, personalizes.
This is where AI becomes genuinely useful in mental health technology. Not as a replacement for clinical judgment, but as a tool for acoustic personalization at scale. The algorithm has one job: to discover, through iterative feedback, what combination of masking, entrainment, and timbral variation works for this particular nervous system on this particular night.
The philosophical stance here is crucial. Sonora does not pretend to diagnose or treat medical conditions. It does not claim to cure tinnitus or anxiety or insomnia. Instead, it positions itself as a tool for acoustic self-regulation—a way of enlisting the brain’s own plasticity in the service of relief.
This is humble. And in a field littered with grandiose mental health apps making unsupported claims, humility is refreshing.
The Philosophy of Free: Why Sonora Stays Open
In 2024, the global wellness app market was valued at approximately $4.2 billion. By 2030, it is projected to exceed $8 billion. Most of this growth is driven by subscription models: Calm, Headspace, Insight Timer, and dozens of competitors lock core features behind paywalls. A person suffering from insomnia can access basic meditations; genuine personalized soundscapes cost $12.99 per month.
This model has generated criticism from neuroscientists and public health researchers. Dr. Felicity Callard at Durham University has argued that the “mindfulness-industrial complex” has transformed a public health issue—the epidemic of sleep loss and anxiety in contemporary life—into a problem of individual consumer choice. If you cannot sleep, the logic goes, it is not the fault of a system that demands constant productivity and connection; it is your failure to pay for the right app.
Sonora was built in explicit rejection of this logic. The app is free. Not freemium—with basic features limited and premium features locked. Entirely free. No ads, no data harvesting, no algorithmic feed designed to maximize engagement and advertising spend. The entire feature set, including adaptive frequency entrainment, personalization, and offline functionality, is available to every user.
This model is sustainable through a different mechanism: direct funding from researchers, sleep medicine clinicians, and a coalition of public health advocates who believe that neurological relief should not be a luxury good. It is funded through grants, not venture capital. It is governed by an open governance board, not a corporate board of directors optimizing for quarterly returns.
The philosophical underpinning is simple: if a tool’s scientific evidence suggests it can help millions of people, and if that tool can be built and distributed at minimal marginal cost (sound files are computationally cheap), then restricting access to those people who can afford it is not sound public health policy. It is triage by wallet.
Sonora’s founders have made a different choice. They have accepted lower financial returns in exchange for maximum reach and maximum impact. In the language of bioethics, they have chosen distributive justice over profit maximization.
This is not idealism divorced from reality. The app works. Users report significant reductions in tinnitus distress, improvements in sleep latency and duration, and decreased anxiety symptoms. Preliminary data suggests efficacy comparable to CBT-I in some cohorts and superior to both placebo and standard sleep medications in others.
And the cost of providing this service to an additional user is, essentially, zero. This is why Sonora remains free. Not out of altruism alone, but out of basic epidemiological logic: a tool that helps millions of people achieve better sleep and lower anxiety, at no financial barrier to entry, is a tool worth maintaining and expanding, regardless of whether it generates venture-scale returns.
10–15%
1 in 4
$0
Cost of Sonora access—entirely free, forever
The Case for Personalized Acoustic Medicine
The conversation around mental health technology often bifurcates into two camps: those who champion digital therapeutics as democratizing mental healthcare, and those who warn that apps cannot replace human connection, clinical expertise, and real structural change.
Both positions contain truth. An app cannot diagnose depression or treat trauma. A soundscape cannot replace cognitive therapy or medical intervention. But this does not mean a soundscape has no role. Medicine works through multiple mechanisms, in layers.
A person with severe insomnia might benefit from therapy, medication, sleep restriction protocols, and environmental design. They might also benefit from a soundscape tailored to their neurotype, played every night, for free, without the friction of subscription management or premium paywalls. These are not contradictory; they are complementary.
Sonora’s vision is precisely this: acoustic support as one tool in a broader ecosystem of wellbeing. Not a replacement for clinical care, but an amplifier of it. A person attending therapy for anxiety can use Sonora’s soundscapes as a between-session tool for nervous system regulation. A person prescribed sleep medication can use Sonora to gradually reduce dosage while maintaining sleep quality. A person with chronic tinnitus can use Sonora daily to lower the threat-level their brain assigns to phantom noise.
The neuroscience suggests this layered approach works. The brain is not a single system; it is a network of overlapping regulatory mechanisms. Sound entrainment works at the level of oscillatory synchronization. Sound masking works at the level of attentional capture. Personalization works at the level of learned association—the brain learns: “this soundscape signals safety; when I hear it, I relax.”
Over weeks and months, these mechanisms cascade. A person uses Sonora nightly for two weeks, and their sleep latency decreases by 15 minutes. By month two, they are not waking at 3 a.m. By month three, they are dreaming again—a sign that the brain has returned to deeper sleep architecture. The nervous system has been gently retrained.
This is not a cure. Tinnitus does not disappear; anxiety does not evaporate. But the relationship to these experiences shifts. They become background noise rather than foreground threat. The sufferer regains agency.
And the cost is zero, the barrier is zero, the friction is zero. You download an app. You choose a soundscape. You press play. That is all.
The Future of Acoustic Science
The early 2020s marked a turning point in sleep and anxiety research: the recognition that the acoustic environment is a modifiable risk factor, not an inevitable consequence of modern life. This shift from acceptance to intervention opened new research frontiers.
The next generation of acoustic interventions will likely integrate real-time biofeedback. Imagine an app that detects your heart rate variability through your phone’s camera, measures your respiratory rate, and in real time adjusts the frequency profile of your soundscape to maximize parasympathetic tone. This technology exists in labs; it is beginning to move into clinical and consumer settings.
Sonora is already exploring such integrations. Early pilots with wearable heart rate monitors suggest that closed-loop biofeedback—where the app continuously monitors your nervous system state and adjusts sound output accordingly—yields even larger effect sizes than static, pre-recorded soundscapes.
The philosophical question remains the same, however: who owns this data? Who benefits from these interventions? Sonora’s answer is clear: the user owns the data; the user benefits from the tool; the platform remains free and open.
In a world where mental health technology has become synonymous with attention capture, data harvesting, and algorithmic manipulation, Sonora stands out not for technical innovation alone, but for philosophical integrity. It asks: what if we built mental health technology not to maximize engagement or profit, but to genuinely serve the people who use it?
What if we acknowledged that nervous system dysregulation—tinnitus, anxiety, insomnia—is a public health crisis, and that people should not have to pay $13 per month for relief?
What if sound, one of the most fundamental human experiences, one that shaped our ancestors’ survival and still shapes our nervous systems today, was treated as a public good rather than a premium service?
Sonora begins to answer these questions, not through rhetoric, but through action: by building, maintaining, and offering, freely and perpetually, a tool that works. That is, in the end, the philosophy behind the app. Not innovation for innovation’s sake. Not profit maximization disguised as wellbeing. But pragmatic, humble, evidence-based service to human flourishing.

