On a quiet night somewhere in Seoul, forty-three volunteers with troubled sleep pressed a set of headphones to their ears and listened to music. For half of them, woven invisibly beneath the melody, two pure tones played simultaneously — one into the left ear, one into the right, separated by exactly six cycles per second. They could not hear the difference. Their brains, it turns out, could.
The study, published in Brain Sciences in 2022 and conducted by researchers at Seoul National University Bundang Hospital, set out to answer a deceptively simple question: can a precisely tuned auditory illusion — a binaural beat — push the waking brain toward sleep? The answer, drawn from the electrical signatures of thought itself, is more nuanced and more promising than either enthusiasts or sceptics might expect.
A Phenomenon Born in the Brainstem
Binaural beats are not a sound you can record with a microphone. They exist only inside the skull. When the left ear receives a tone of, say, 256 Hz and the right ear receives 262 Hz, the brain perceives a phantom oscillation at the difference frequency — in this case, 6 Hz. The processing takes place not in the auditory cortex but in the medial superior olivary nucleus of the pons, a brainstem structure that normally helps localise sound in space by comparing the timing of signals from both ears.
What makes binaural beats medically interesting is a concept called entrainment, or the frequency-follow response. The brain’s electrical activity — its native rhythms of delta, theta, alpha and beta — has a tendency to synchronise with repetitive external stimuli. Drummers know this empirically. Monks have exploited it for millennia. The question science has been circling is whether a digital audio file can do the same thing reliably, measurably, in a clinical population.
“When the participants listened to music with binaural beats, the relative power of the theta wave increased. The brain, it seems, was listening more carefully than its owner.”Brain Sciences, 2022 — Yoon, Bae & Cho et al.
Mapping the Insomniac Brain
Insomnia is not simply a failure to fall asleep. At its neurological root lies a state of cortical hyperarousal — an excess of high-frequency beta activity that keeps the brain in a state of alert wakefulness when the body has long since collapsed with fatigue. The resting EEG of a chronic insomniac looks, in certain respects, like the EEG of someone doing mental arithmetic. The lights will not go out.
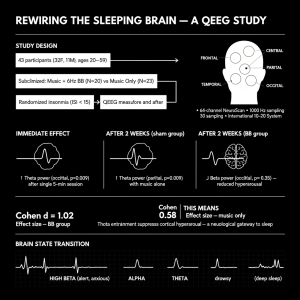
The Seoul team recruited forty-three adults between the ages of twenty and fifty-nine with subclinical insomnia — people who lay awake far too long, woke too easily, and emerged from sleep feeling cheated, but whose symptoms fell short of the full diagnostic threshold for insomnia disorder. Their baseline Pittsburgh Sleep Quality Index scores averaged 8.7, well above the clinical cut-off of five. Crucially, none were taking sleep medications.
Participants were randomised into two groups. Both received an audio device and instructions to listen for thirty minutes before bed every night for two weeks. The test group’s device played music embedded with a 6 Hz binaural beat — a theta-frequency stimulus, targeting the brain rhythm most closely associated with drowsiness and the hypnagogic state at the edge of sleep. The control group’s device played identical music, with the binaural tone stripped silently away.
What the Electrodes Recorded
To measure brain activity, researchers used a 64-channel quantitative electroencephalography system — essentially a swimming cap studded with electrodes, each recording the summed electrical chatter of millions of neurons below the scalp. Measurements were taken in a laboratory, twice: before the two-week intervention, and after. Fast Fourier transformation converted the raw EEG signal into a spectral map, revealing the relative power of each frequency band across five anatomical regions of the cortex.
The first finding arrived quickly. Before the two-week protocol even began, simply listening to music with a binaural beat for five minutes produced a measurable increase in theta power at the occipital region, at the back of the skull (p = 0.009). No equivalent shift was seen in the control condition. The brain was, apparently, following the rhythm within a single session.
After two weeks, the picture became more layered. Among those who had been using the binaural beat device at home, exposure to music with the beat in the laboratory produced elevated theta power at the parietal region (p = 0.009). More strikingly, the group that had listened to music with binaural beats for a fortnight showed a significantly greater reduction in beta power from baseline — the very signature of cortical hyperarousal — compared to the music-only group (p = 0.035, occipital region).
The Architecture of Drowsiness
To appreciate what a beta reduction means, it helps to understand the EEG landscape of falling asleep. In a healthy sleeper, the transition from wakefulness to Stage 1 sleep follows a characteristic choreography. Alpha waves — the 8 to 12 Hz oscillations of relaxed, eyes-closed wakefulness — begin to yield. Theta activity rises in the frontal and parietal regions. Beta power falls. The brain, in electrical terms, is dimming its lights. In the chronic insomniac, this transition is impeded; beta persists, alpha spikes, and the sleeper remains stranded in a neurological no-man’s-land.
The Seoul data suggest that binaural beat stimulation may be capable of nudging the brain toward exactly this transition. The selective increase in theta power, combined with the reduction in beta, traces the first steps of the dimming sequence. The effect size in the binaural beat group — Cohen’s d of 1.02, compared to 0.58 in the music-only arm — represents a clinically meaningful difference, even if the small sample prevented the broader symptom questionnaire scores from reaching statistical significance.