
The Beat You Cannot Hear — and Why It May Change How We Sleep

Petr Barák
author, designer
A new generation of auditory science is challenging the pharmaceutical dominance of the sleep industry. Dynamic binaural beats — engineered illusions born inside the brain itself — are emerging as a credible, drug-free route into deeper, faster, more restorative sleep.
21 March 2026 6 min read
There is no sound. That is, perhaps, the most startling thing about binaural beats: the tone that supposedly reshapes your brain activity does not exist anywhere in the physical world. It is generated entirely within the auditory cortex — an acoustic hallucination conjured by the gap between two almost-identical frequencies, one delivered to each ear. Send 100 hertz to the left ear and 103 hertz to the right, and the brain, bridging the difference, perceives a third tone pulsing at three cycles per second. It is an illusion, yes. But its effects on neural activity, researchers now argue, may be quite real.
For more than three decades, binaural beats have occupied an ambiguous middle ground between serious neuroscience and the more credulous margins of wellness culture. They have been championed on late-night radio programmes, sold on relaxation apps and dismissed, repeatedly, by researchers who found their effect sizes modest or their study designs wanting. Yet the science has not stood still. A new class of auditory stimulation — dynamic binaural beats, or DBB — has introduced a key refinement that its proponents believe addresses many of the methodological failings of earlier work. The early results are difficult to ignore.
The Mechanism
To understand why dynamic binaural beats represent an advance, one must first understand what made the original concept so theoretically compelling. The brain’s electrical activity can be broadly characterised by its dominant frequency at any given moment. During deep, dreamless sleep, it slows to the delta band: somewhere between 0.5 and 4 hertz. As we drift into drowsiness, theta waves — four to eight hertz — take over, the same frequencies associated with meditative states and the hypnagogic borderland between waking and sleep. Alert cognition rides on beta waves; focused calm on alpha. The brain, in other words, is a tunable instrument, and its tuning reflects, in measurable terms, the quality of consciousness at any instant.
The hypothesis underlying binaural beat therapy is straightforward: if the brain can be induced to follow an external oscillatory signal — a phenomenon known as neural entrainment — then a listener wearing headphones might guide their own brainwaves toward the frequencies of sleep. Present a delta-frequency beat during the pre-sleep period, the theory goes, and the cortex will begin to oscillate in sympathy.
“The tone that reshapes your brain activity does not exist anywhere in the physical world. It is generated entirely within the auditory cortex — an acoustic hallucination conjured by the gap between two almost-identical frequencies.”
— Sonora Science Desk
Static binaural beats — where the carrier frequency remains fixed throughout the listening session — have shown mixed results in clinical literature. Some studies demonstrate reductions in anxiety and improvements in subjective sleep quality; others find no significant difference from silence or sham conditions. Critics have pointed to small sample sizes, inconsistent delivery methods and a failure to account for habituation: the brain’s tendency to stop responding to a stimulus once it becomes sufficiently familiar. A tone that is perpetually identical may, in time, become neurologically invisible.
The Dynamic Difference
It is here that the work published in Sleep, the journal of the Sleep Research Society, in April 2024, makes its most significant contribution. A team of researchers — led by Hwa-Ah-Ni Lee and colleagues at Korea University — introduced a variant they termed dynamic binaural beats, which incorporates a continuously modulating carrier frequency. In their protocol, the right ear received a tone that shifted between 100 and 103 hertz over a defined period, while the left ear remained fixed at 100 hertz. The perceived beat frequency therefore ranged from zero to three hertz — traversing the lower boundary of delta across a gradient, rather than locking onto a single target.
The logic is elegant. If the brain’s tendency toward habituation is the principal obstacle to entrainment, a moving target should preserve the novelty — and therefore the neurological salience — of the stimulus. Rather than a hammer striking the same note repeatedly, DBB acts more like a hand drawn slowly across the keys of a piano: the brain must track, adjust and follow, maintaining its engagement throughout.
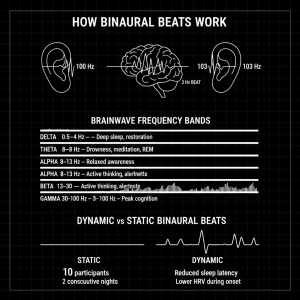
Fig. 1 — How binaural beats are generated, the five canonical brainwave frequency bands, the distinction between static and dynamic delivery, and key findings from Lee et al. (2024). Graphic: malbardesign.com / AI
The study enrolled ten healthy participants in a cross-over design, meaning each volunteer experienced both the DBB condition and a sham condition — absence of sound — across two consecutive nights, with full polysomnography evaluation throughout. The DBB was administered during three specific windows: the pre-sleep initiation period, sleep onset, and the transition from rapid eye movement sleep back to non-REM stages. The results were striking in their consistency.
10 Healthy participants in crossover design
0–3 Hz Dynamic beat frequency range (delta band)
↓ HRV Reduced heart rate variability during sleep onset
Dynamic binaural beats significantly reduced sleep latency — the time taken to fall asleep — compared with the sham condition. Electrocardiogram analysis revealed that exposure to DBB led to diminished heart rate variability during both the pre-sleep initiation and sleep onset periods, accompanied by a decrease in low-frequency power of heart rate during sleep onset. Heart rate variability is widely regarded as a proxy for autonomic nervous system activity: lower values during sleep onset suggest a shift toward parasympathetic dominance — the physiological state associated with relaxation, recovery, and the body’s preparation for deep rest. In practical terms, the heart was slowing, the nervous system was quieting, and sleep was arriving sooner. “DBB might be effective in improving sleep quality,” the authors concluded, “suggesting its possible application in insomnia treatments.”
A Broader Context
The Lee et al. study arrives against a backdrop of growing clinical interest in non-pharmacological sleep interventions. The global insomnia epidemic — affecting an estimated ten to thirty per cent of adults in developed nations — has for decades been managed primarily with benzodiazepines and their successors: medications that knock the brain offline rather than guiding it into natural sleep architecture. The distinction matters enormously. Drug-induced sleep suppresses REM activity, shortens the deeper restorative stages and carries well-documented risks of dependency, tolerance and cognitive hangover. The appeal of any intervention that works with the brain’s own oscillatory logic, rather than overriding it, is therefore considerable.
Prior research has established a modest but credible evidence base for binaural beat therapy in adjacent domains. A 2023 study published in PMC found that theta-frequency binaural beats — targeting the four-to-eight hertz band — showed efficacy in altering brainwave patterns in insomnia sufferers, improving both subjective sleep quality scores and objective electroencephalographic markers. A separate randomised controlled trial examining delta binaural beats in overworked employees reported improvements in sleep quality and reductions in depressive mood. The picture that emerges, across this body of work, is not one of miracle treatment but of a measurable, repeatable physiological nudge — one that may be most powerful when the delivery method is refined.
That refinement is precisely what the dynamic approach attempts to provide. A systematic review published in PLOS ONE — one of the more rigorous meta-analyses of the field — found that while the evidence for binaural beat entrainment remained mixed, the most consistent results clustered around protocols that maintained sustained attention from the auditory cortex. Monotony, the reviewers suggested, was the enemy of entrainment. The dynamic modulation built into DBB is, by this logic, not merely an incidental variation but a theoretically motivated design choice targeting the core weakness of the first generation of research.
“Drug-induced sleep suppresses REM activity and shortens the deeper restorative stages. The appeal of any intervention that works with the brain’s own oscillatory logic — rather than overriding it — is therefore considerable.”
— Sonora Science DeskWhat Remains Unknown
Scientific honesty requires that the limitations of this emerging field be stated plainly. The Lee et al. proof-of-concept study enrolled ten participants — a sample size adequate for preliminary signal detection but wholly insufficient for the kind of statistical confidence that clinical translation demands. The crossover design, while elegant in controlling for individual variability, cannot account for order effects or the possibility that the sham condition itself — enforced silence during the pre-sleep period — may have influenced results through expectation or the absence of ambient sound. The study’s authors are admirably candid about these constraints, framing their findings explicitly as a proof of concept that warrants larger, more rigorously controlled trials.
There are also deeper questions about mechanism that the field has yet to resolve. Neural entrainment — the idea that the brain will synchronise its electrical oscillations to an external periodic stimulus — is well established for visual and tactile inputs. For auditory binaural beats, the evidence of genuine cortical entrainment, as opposed to a more diffuse change in arousal state, remains contested. Some neuroimaging studies have identified increased power in the relevant frequency bands following binaural beat exposure; others have not replicated these findings. It is possible that the cardiovascular and subjective sleep benefits observed in the DBB research reflect not direct cortical entrainment but a more indirect pathway — perhaps mediated by autonomic nervous system calming, auditory distraction from anxious thought, or simple relaxation response triggered by any consistent sound stimulus.
None of this is fatal to the enterprise. The clinical question — does this help people sleep, and does it do so safely? — is ultimately separable from the mechanistic question of precisely how. Sleep medicine has a long tradition of using interventions whose mechanisms are incompletely understood, from melatonin to cognitive behavioural therapy for insomnia. What matters, at the level of the individual patient lying awake at three in the morning, is whether the intervention works.
Looking Ahead
The trajectory of dynamic binaural beat research over the next five years will likely be shaped by three converging forces. First, the proliferation of consumer wearables capable of real-time electroencephalographic and heart rate monitoring makes it increasingly feasible to deliver closed-loop DBB protocols — systems that adjust the frequency parameters of the auditory stimulus in response to the listener’s live biosignal data, rather than following a pre-programmed schedule. A beat that adapts to where your brain actually is, rather than where a protocol assumes it should be, represents a qualitatively different kind of intervention. Several research groups are already exploring this adaptive paradigm.
Second, the growing clinical appetite for non-pharmacological sleep interventions — driven partly by regulatory pressure on long-term sedative prescribing and partly by a generational shift in patient attitudes toward medication — creates a receptive environment for validated audio-based therapies. If larger trials replicate the Lee et al. findings with adequate statistical power, the route to clinical adoption in sleep medicine settings is not implausible within a decade.
Third, the commoditisation of high-fidelity audio technology means that the barriers to access are lower than for almost any other medical intervention. A pair of headphones and a carefully engineered audio file are, in cost terms, accessible to virtually any patient. The equity implications of a clinically validated, inexpensive sleep therapy are significant in an era when insomnia disproportionately afflicts lower-income populations with the least access to specialist care.
For now, the prudent position is one of cautious optimism. Dynamic binaural beats have cleared the first hurdle: they have demonstrated a plausible, measurable signal in a controlled setting. The ears are open. The question is whether the science, with the rigour of larger trials and the ingenuity of adaptive delivery, can justify the promise of what that signal might ultimately mean for the tens of millions who lie awake each night, waiting for sleep that refuses to come.
Sources & References
- Lee, H.A. et al. (2024). “Effect of dynamic binaural beats on sleep quality: a proof-of-concept study with questionnaire and biosignals.” Sleep, 47(10), zsae097. DOI: 10.1093/sleep/zsae097
- Bavafa, A. et al. (2023). “Investigating the Efficacy of Theta Binaural Beat on the Sleep Quality of Patients with Insomnia.” PMC / PubMed Central, PMID 38077174.
- Dabiri, R. et al. (2022). “The effect of auditory stimulation using delta binaural beats on sleep and depressive mood among overworked employees: A randomised-controlled clinical trial.” Digital Health, SAGE Journals. DOI: 10.1177/20552076221102243
- Askarpour, H. et al. (2024). “Binaural Beats’ Effect on Brain Activity and Psychiatric Disorders.” Open Public Health Journal, Vol. 17.
- Garcia-Argibay, M., Santed, M.A., & Reales, J.M. (2019). “Binaural auditory beats affect long-term memory.” Psychological Research.
- Clinicaltrials.gov. (2024). “Improvement of Sleep Quality of Insomnia Patients with Binaural Beats.” NCT06604208.


